Overview
 Bunions are common but they can be misdiagnosed. We sometimes assume that any lump at the bottom of the big toe is a bunion. But as the Latin name (hallux valgus) suggests, the hallmark of a bunion is what happens to the toe itself (the hallux) rather than to the joint at its base. In bunions, the toe veers off in a valgus direction, that is, away from the midline. An outcrop of extra bone, or osteophyte, develops as the body tries to protect the exposed surface of the warped first metatarsophalangeal joint (MTP); a fluid-filled sac, or bursa, may also form, which often becomes inflamed. Foot experts are still not entirely agreed about what causes bunions. Genetics and lax ligaments are both implicated; the role of footwear is less clear. All bunion conversations seem to involve someone stating that barefoot tribes people don?t get bunions. This is not true.
Bunions are common but they can be misdiagnosed. We sometimes assume that any lump at the bottom of the big toe is a bunion. But as the Latin name (hallux valgus) suggests, the hallmark of a bunion is what happens to the toe itself (the hallux) rather than to the joint at its base. In bunions, the toe veers off in a valgus direction, that is, away from the midline. An outcrop of extra bone, or osteophyte, develops as the body tries to protect the exposed surface of the warped first metatarsophalangeal joint (MTP); a fluid-filled sac, or bursa, may also form, which often becomes inflamed. Foot experts are still not entirely agreed about what causes bunions. Genetics and lax ligaments are both implicated; the role of footwear is less clear. All bunion conversations seem to involve someone stating that barefoot tribes people don?t get bunions. This is not true.
Causes
While the precise cause is not known, there seem to be inherited (genetic) factors that lead to abnormal foot function like overpronation that can predispose to the development of bunions. This is especially common when bunions occur in younger individuals. This abnormal biomechanics can lead to instability of the metatarsal phalangeal joint and muscle imbalance resulting in the deformity. Although shoe gear doesn't directly cause a bunion, it can certainly make the bunion painful and swollen. Other less common causes of bunion deformities include trauma (sprains, fractures, and nerve injuries), neuromuscular disorders (polio or Charcot-Marie-Tooth disease) and limb-length discrepancies (one leg shorter than the other) where the longer leg develops the bunion.
Symptoms
Look for an angular, bony bump on the side of the foot at the base of the big toe. Sometimes hardened skin or a callus covers this bump. There's often swelling, redness, unusual tenderness, or pain at the base of the big toe and in the ball of the foot. Eventually, the area becomes shiny and warm to the touch. Seek medical advice if you have persistent pain when walking normally in otherwise comfortable, flat-soled shoes, you may be developing a bunion, bursitis, or a bone spur in your foot.
Diagnosis
A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen.
Non Surgical Treatment
You can try over-the-counter remedies like pads to stop them rubbing, or take painkillers such as paracetamol or ibuprofen if they play up. Devices that fit into your shoe, called orthotics, or splints that you wear at night, can slow the progression of bunions. If these don't help and the bunion is causing a painful and substantial deformity that?s seriously limiting your footwear, your GP will probably refer you to see a podiatrist, medical professionals who specialise in feet. They can give further advice about non-invasive treatments and also refer you for an operation, either with a podiatric or orthopaedic (bone) surgeon, ultimately the only thing that can correct the gnarly blighters. You can visit a podiatrist privately, which will cost anything from ?140-?200. But Mike O?Neill, spokesperson for the Society of Podiatrists and Chiropodists, suggest always going via your GP, who will know the best qualified. Such is the complexity of the bone structure of the foot, there are more than 130 different surgical procedures for bunions. One person?s op may be very different from another?s, so be wary of sounding out a friend about theirs.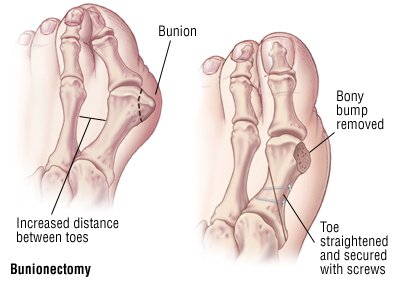
Surgical Treatment
One of the more popular proximal metatarsal osteotomies that is performed is called the Myerson/Ludloff procedure. This operation is performed for more advanced deformity. Screws are inserted into the metatarsal to hold the bone cut secure and speed up bone healing. Walking is permitted in a surgical shoe following surgery. The shoe is worn approximately 5 weeks.
Bunions are common but they can be misdiagnosed. We sometimes assume that any lump at the bottom of the big toe is a bunion. But as the Latin name (hallux valgus) suggests, the hallmark of a bunion is what happens to the toe itself (the hallux) rather than to the joint at its base. In bunions, the toe veers off in a valgus direction, that is, away from the midline. An outcrop of extra bone, or osteophyte, develops as the body tries to protect the exposed surface of the warped first metatarsophalangeal joint (MTP); a fluid-filled sac, or bursa, may also form, which often becomes inflamed. Foot experts are still not entirely agreed about what causes bunions. Genetics and lax ligaments are both implicated; the role of footwear is less clear. All bunion conversations seem to involve someone stating that barefoot tribes people don?t get bunions. This is not true.Causes
While the precise cause is not known, there seem to be inherited (genetic) factors that lead to abnormal foot function like overpronation that can predispose to the development of bunions. This is especially common when bunions occur in younger individuals. This abnormal biomechanics can lead to instability of the metatarsal phalangeal joint and muscle imbalance resulting in the deformity. Although shoe gear doesn't directly cause a bunion, it can certainly make the bunion painful and swollen. Other less common causes of bunion deformities include trauma (sprains, fractures, and nerve injuries), neuromuscular disorders (polio or Charcot-Marie-Tooth disease) and limb-length discrepancies (one leg shorter than the other) where the longer leg develops the bunion.
Symptoms
Look for an angular, bony bump on the side of the foot at the base of the big toe. Sometimes hardened skin or a callus covers this bump. There's often swelling, redness, unusual tenderness, or pain at the base of the big toe and in the ball of the foot. Eventually, the area becomes shiny and warm to the touch. Seek medical advice if you have persistent pain when walking normally in otherwise comfortable, flat-soled shoes, you may be developing a bunion, bursitis, or a bone spur in your foot.
Diagnosis
A doctor can very often diagnose a bunion by looking at it. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen.
Non Surgical Treatment
You can try over-the-counter remedies like pads to stop them rubbing, or take painkillers such as paracetamol or ibuprofen if they play up. Devices that fit into your shoe, called orthotics, or splints that you wear at night, can slow the progression of bunions. If these don't help and the bunion is causing a painful and substantial deformity that?s seriously limiting your footwear, your GP will probably refer you to see a podiatrist, medical professionals who specialise in feet. They can give further advice about non-invasive treatments and also refer you for an operation, either with a podiatric or orthopaedic (bone) surgeon, ultimately the only thing that can correct the gnarly blighters. You can visit a podiatrist privately, which will cost anything from ?140-?200. But Mike O?Neill, spokesperson for the Society of Podiatrists and Chiropodists, suggest always going via your GP, who will know the best qualified. Such is the complexity of the bone structure of the foot, there are more than 130 different surgical procedures for bunions. One person?s op may be very different from another?s, so be wary of sounding out a friend about theirs.
Surgical Treatment
One of the more popular proximal metatarsal osteotomies that is performed is called the Myerson/Ludloff procedure. This operation is performed for more advanced deformity. Screws are inserted into the metatarsal to hold the bone cut secure and speed up bone healing. Walking is permitted in a surgical shoe following surgery. The shoe is worn approximately 5 weeks.
 RSS Feed
RSS Feed
